Tension headaches are caused by muscle tension in the scalp, forehead, and back of the neck. A tension-type headache is the most common type of headache, yet its causes aren't well understood. Several causes of headaches are known, but the exact cause is unknown. Here we will be discussing in depth about tension headaches in order to provide you with a better understanding.
Published on
•
Slug
tension-type-headache
Video
CoverSVG
Category
Headache
Excerpt
Tension headaches are caused by muscle tension in the scalp, forehead, and back of the neck. A tension-type headache is the most common type of headache, yet its causes aren't well understood. Several causes of headaches are known, but the exact cause is unknown. Here we will be discussing in depth about tension headaches in order to provide you with a better understanding.
The most prevalent type of headache is tension headache. Some people only have tension headaches once or twice a year, while others suffer from them on a daily basis. During times of stress, they may appear more frequently than usual. Despite their discomfort, most people can go about their daily routines despite a tension headache if left untreated.
People don't usually go to the doctor when they have a stress headache, making exact figures difficult to forecast. Research suggests that one in every three adults in the United States suffers from tension headaches. It is the most common type of headache experienced by children.
Key Points:
It was found that 79% of patients had TTH at some point in their lifetime, with 3% experiencing CTTH (i.e. headache occurring on more than 15% of the days per month). It seems that TTH occurs more in women than in men, and it declines with age for both sexes.
With TTH, women are only slightly more likely to suffer (the female-to-male ratio is 5:4) and the onset period (25 to 30 years) is delayed compared to migraine.
As one age, there is a slight decrease in prevalence, which occurs most commonly between ages 30 to 39.
Types of Tension-type headache
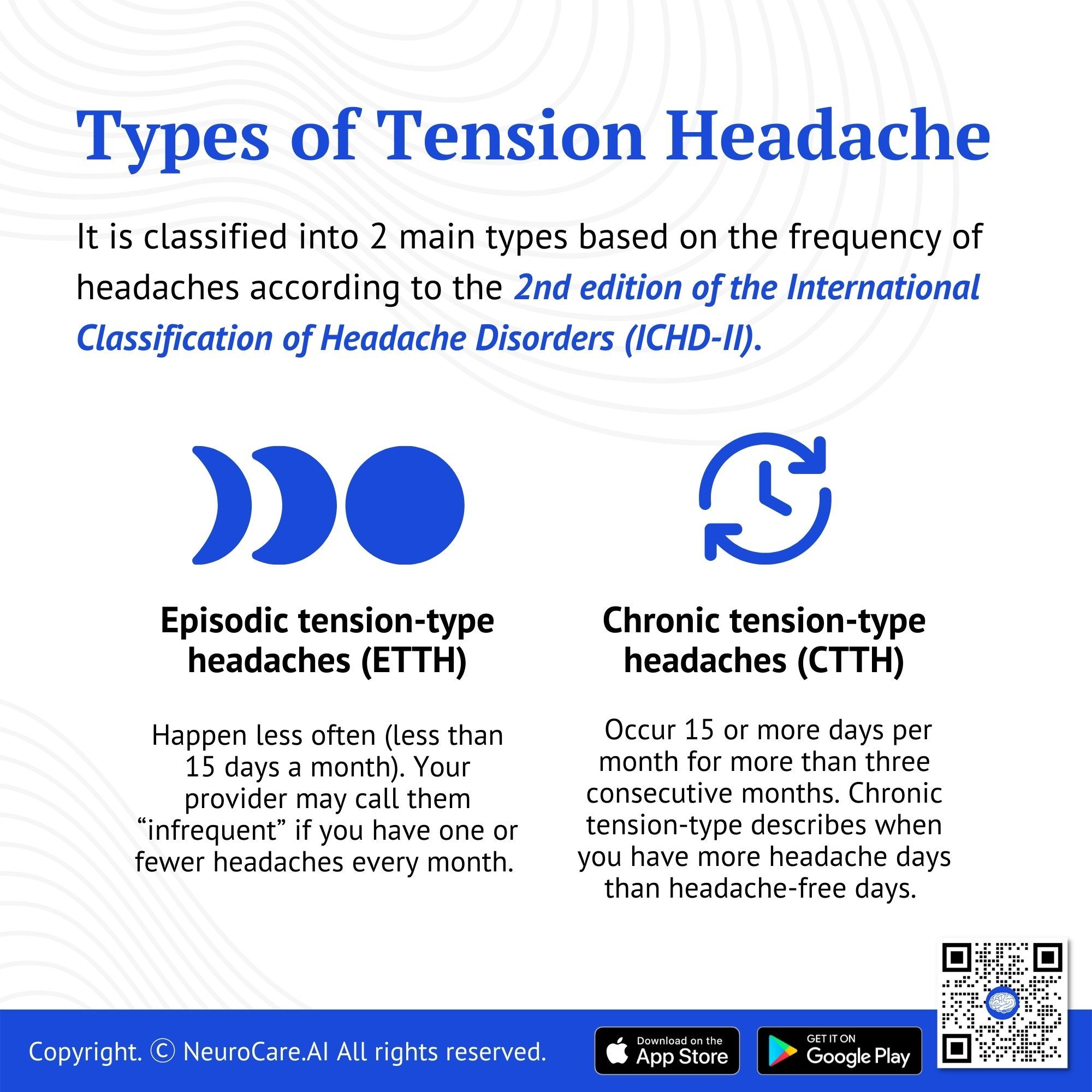
It is classified into 2 main types based on the frequency of headaches according to the 2nd edition of the International Classification of Headache Disorders (ICHD-II).
Episodic tension-type headaches (ETTH)
Episodic tension-type headaches happen less often (less than 15 days a month). Your provider may call them “infrequent” if you have one or fewer headaches every month.
Can be an infrequent or frequent episodic headache.
The infrequent type occurs once or twice a month.
The frequent type occurs less than 15 days per month.
At least 10 episodes occur more than 1 day and less than 15 days per month for at least 3 months.
It usually starts slowly and progresses throughout the day.
It can last from 30 minutes to a week.
Chronic tension-type headaches (CTTH)
Chronic tension-type describes when you have more headache days than headache-free days. Chronic tension headaches occur 15 or more days per month for more than three consecutive months.
Occurs more than 15 days a month for at least 3 months consecutively.
It starts slowly and lasts for days. The pain can exacerbate or ease as the day progresses, but it is always there.
More than 180 days/year
What Causes Tension-Type Headaches?
Several causes of headaches are known, but the exact cause is unknown. Emotional tension or stress may be a factor. Several causes of headaches are known, but the exact cause is unknown. Emotional tension or stress may be a factor. Tension headaches are believed to be caused by muscle tension in the scalp, forehead, and back of the neck. This can be triggered by:
tension and stress,
tiredness,
long periods of reading, typing, or concentration (eye strain),
poor posture,
spine and neck injuries,
high blood pressure, and
physical or emotional stress.
Some people believe that certain things cause headaches. Some foods, intense sunlight, disease, depression, anxiety, cold, heat, exhaustion, noise, alcohol, caffeine, and so on are examples. However, many headaches develop for no apparent reason.
Medication is a special cause of frequent headaches.
It is possible to cause headaches by overusing painkillers for headaches. If this occurs, it may induce a vicious cycle. If you are experiencing a bad spell of headaches, you may take regular painkillers. As time passes, you may even find yourself taking painkillers on a daily basis. Your body will then get used to taking them on a regular basis. It is important to note, however, that if painkillers are not taken every day, then a 'rebound headache' forms. Three out of every hundred people suffer from headaches most of the time. One of the main causes of headaches is the use of painkillers on a daily basis. Sometimes headaches are caused by side effects of medications used to treat other conditions such as heart conditions.
🧠 Insights: There is growing evidence that emotional disturbances may increase the risk of TTH. Stress and mental tension are the most common causes of TTH and in patients with TTH, headaches have been shown to be positively correlated with stress. It has been proven that chronic recurrent headaches, mainly chronic tensional headaches (CTTH), are associated with an increase in the frequency and severity of minor life events as well as daily hassles.
Clinical Features
General Symptoms
A tension headache is often described as a headache in the "hat-band" area. People sometimes feel a "pinch" or "pressure" in their heads. Usually, both sides of the head are affected, as well as the neck. Occasionally it affects just one side. There may occasionally be tenderness on the scalp and jaw pain. This may last for 30 minutes to 7 days. It usually lasts for a few hours. People with moderate or mild severity can also have severe cases. As opposed to migraine headaches, tension headaches are usually less severe and more constant than throbbing headaches. There are usually no other symptoms associated with tension headaches.
Pain. Most people describe TTH pain as dull, pressure-like, constricting, or giving them a feeling of fullness in the head. It is not uncommon for patients to describe their pain as being like wearing a tight hat or wearing a tight band around their head, or bearing a heavy burden. A majority of patients do not believe that physical activity affects their headache intensity. This is in stark contrast to migraine in which the pain worsens with routine physical activity, and it is therefore considered one of the best criteria for distinguishing migraine from TTH. In 90% of cases, TTH patients experience bilateral pain. However, the location of the pain varies considerably and can be either posterior or anterior.
Accompanying clinical features. Symptoms associated with nausea and vomiting rule out tension headache. However, about 20% of TTH patients may suffer from mild-to-moderate anorexia (as defined by the ICHD II criteria), which should not be confused with nausea. It is possible to have either phobic or photophobic symptoms, but the presence of both symptoms is not permitted.
Exacerbating factors and precipitating factors. Lack of sleep, stress, and forgetting to eat are among the most common headache-triggering factors reported by both migraineurs and people with tension headaches. Occasionally, alcohol and menstruation can also trigger headaches in patients with ETTH. A significant number of ETTH patients report aggravating conditions that commonly aggravate established headache attacks in migraine patients. These factors do not provide much useful information to distinguish TTH from migraine, although they may influence treatment.
Diurnal variations. Generally, TTH is reported to begin during the day and to increase slowly. Afterward, the headache usually persists throughout the day and is often unaffected by wide-ranging activities, although some people may notice an aggravation by evening.
Physical Examinations - The diagnosis of TTH requires the exclusion of other causative disorders, so a thorough clinical history is required as well as a careful physical and neurological examination. In the physical examination, tender points and trigger points should be identified by palpating pericranial muscles.
Tender points are areas where manual pressure induces local pain; and
Trigger points tenderness that induces referred pain in another part of the region from localized deep tenderness.
Complications
Over-reliance on non-prescription caffeine-containing analgesics
Dependence on/addiction to narcotic analgesics
GI bleed from the use of NSAIDs
Risk of epilepsy 4 times greater than that of the general population
Medication overuse headache
The overall quality of life is compromised
Absence from school and work
Decreased productivity at work
Inability to take part in physical activities
Treatment
Pharmacological Treatment
Acute (abortive) pharmacotherapy
Studies have been conducted on anti-inflammatory drugs and simple analgesics for treating TTH, using headache attacks as models for acute pain. According to the International Headache Society, NSAIDs are the first-line drugs of choice in studies of TTH. Some studies followed the recommendations for drug trials.
Pain relievers such as paracetamol or aspirin are commonly used and are often effective. It's best to take a pain reliever as soon as a headache starts to develop. This can "drive away" the headache more effectively than treating it once it has fully developed. A second dose of aspirin or paracetamol can be taken 4 hours later if needed. (Pills combined with a small amount of codeine such as co-codamol are best for avoiding headaches. They are more likely to cause "rebound" or drug-induced headaches as described above).
Anti-inflammatory pain relievers are an alternative. One example is ibuprofen. This medication can be purchased from pharmacies, but a prescription is required elsewhere. Anti-inflammatory drugs may be slightly more effective than paracetamol or aspirin. However, side effects such as an upset stomach are sometimes a problem. Always read the leaflet that comes with the anti-inflammatory medication. They may not be recommended for people with other medical conditions such as duodenal ulcers or asthma.
💡 Note: Painkillers for headaches should not be taken for more than a few days at a time. They should not be used more than 15 days per month. More than that can lead to the drug-induced headaches described above. Don't have to take a pain reliever all the time to stop a headache. Do it every day as it comes. See your doctor if you need a daily pain reliever for your headache.
Pharmacological prophylactic pharmacotherapy
Prophylactic therapy is recommended for patients who suffer from frequent episodes of tension headaches or do not respond adequately to acute treatment. It is especially important to initiate prophylactic therapy promptly in patients with frequent headaches since headaches may subsequently increase exponentially and the effectiveness of prophylactic therapy may be reduced by frequent use of acute medications. It's still unknown if treatment can stop or delay the progression of infrequent tension-type headaches to chronic tension-type headaches. Moreover, a review found no prophylactic effect of antidepressants. Due to this, and also adverse effects, if there is no response, it must be decided whether to continue treatment for three months (6 months is the longest) or discontinue it (grade A recommendation).
As one of the most researched prophylactic agents for chronic tension-type headaches, Amitriptyline (Elavil) has received a great deal of attention. This drug is typically used in dosages of 10 to 75 mg before bed to minimize the drowsiness associated with waking up in the morning.
Non-Pharmacological Treatment
In the management of TTH, relaxation, and electromyography (EMG) biofeedback therapies are well supported by science. Together, relaxation training and EMG biofeedback training result in a nearly 50% reduction in headache activity. The improvement rates are similar for each modality but statistically higher than those observed in untreated patients or patients with false or non-contingent biofeedback. It appears that the two treatments are not interchangeable: patients who do not respond to relaxation training can benefit from subsequent EMG biofeedback training.
Relaxation: Different people find different things helpful. For example, walking, exercising, or taking a break from your normal routine can help. Massaging the shoulder and neck muscles is often helpful. Applying a warm flannel to your neck or taking a warm bath may help.
Prophylactic non-pharmacotherapy - It is the aim of prophylactic non-pharmacotherapy to reduce headaches by combining several different modalities such as electromyographic biofeedback, physical therapy, acupuncture, and exercise therapy (exercise that relaxes the neck muscles and occipital muscles), psychotherapy, and lifestyle counseling in order to reduce headaches.
Biofeedback - These are just some of the behavioral medicine techniques proven to relieve headaches and improve functioning, including biofeedback and progressive muscle relaxation. By combining regular use with preventative medication and optimal acute therapy, quality of life is significantly improved compared to medication alone.
Lifestyle
Living a healthy lifestyle can help you feel better in general and may even prevent headaches. Here are some tips to help you get started.
Get enough sleep. Research has shown that getting enough sleep can reduce the frequency and severity of headaches, while too little or too much sleep can increase them.
Don't smoke. Smoking has been linked to many different health problems, including heart disease and cancer, but it also contributes to headaches in smokers and non-smokers alike. If you smoke, it's time to quit!
Exercise regularly. Getting regular exercise helps reduce stress levels and maintain blood pressure within normal limits, which means less risk for headaches!
Shift to a regular, balanced meal. Eating right is key when it comes to staying healthy—and eating regularly throughout the day will help keep your blood sugar levels steady so that cravings don't drive you crazy (or send your head into overdrive).
Rehydrate. Drink plenty of water. Water helps flush toxins out of your system and keeps your organs functioning properly, which will help prevent headaches too!
Prevention
Diary/Journaling. A headache journal diary can be helpful if headaches are frequent. Note when, where, how severe the headache occurs, and for how long. Also, be aware of anything that may have caused it. A trend can emerge and a trigger can be identified. For example, if they seem to appear in direct sunlight, when tired or hungry. Situations that cause eye strain, poor neck posture, stress, anxiety, anger, or other emotions can be identified as headache triggers. Headache situations can be avoided or modified.
Avoid stressful situations whenever possible. It is common for headaches to be caused by stress. Sometimes we are stressed without realizing it. Sometimes a stressful job or situation cannot be avoided. Relaxation exercises can help you cope with stress. Stress can be reduced using breathing exercises or coping strategies. You can buy books (and tapes) on relaxing, and sometimes you may be referred to a counselor or psychologist for help.
Regular exercisecan reduce stress and tension. This can work to relieve occasional headaches. Moderate exercise for 30 minutes at least 3 times a week is best. However, any increase in exercise can be beneficial.
Depression can lead to frequent headaches, and if you suspect this, talk to your doctor.
Preventive medicine may be consulted.These are different from pain relievers and must be taken daily. These include some antidepressants and beta-blockers. They work best for migraines, but may also help some people with frequent tension headaches.
When to See a Doctor
See your local doctor or return to the local 911 Emergency Department if:
You get a headache that is severe and ‘out of the blue’ (a sudden onset).
The pain is worse when you cough, sneeze or strain.
The pain is getting worse, despite taking pain relief.
The pain is worse when you lie down.
You become drowsy, or confused.
Your vision becomes blurred, or you have any visual disturbance.
You are generally unwell, including vomiting.
DISCLAIMER:
The information in this document is for general educational purposes only. It is not intended to substitute for personalized medical professional advice. NeuroCare.AI makes every effort to provide accurate and timely information, but makes no guarantee in this regard and disclaims responsibility for adverse consequences resulting from its use. For further information, consult a physician and the organization referred to herein.
Discover the power of our ambient clinical documentation system, designed to transform clinical encounters into structured SOAP notes with unmatched ease. Experience exceptional value for less than $3 per day—cheaper than your daily coffee!
Save Time: Free up over 90 minutes daily for each provider.
Boost Revenue: Increase daily revenue by at least $1,000 per provider.
Maximize Engagement and Interaction: Dedicate more time to patient care and less to typing, fostering richer and more effective conversations between clinicians and patients
Discover our breakthrough Radiology AI reporting platform built on Ambient AI. It enhances productivity and minimizes fatigue. Benefit from best-in-class accuracy with our automated radiology report generation, all at market-leading pricing.
📈 Efficiency: Cut dictation times by up to 50% (Less words, More report!
🎯 Focus: Keep your eyes on the images, not the keyboard!